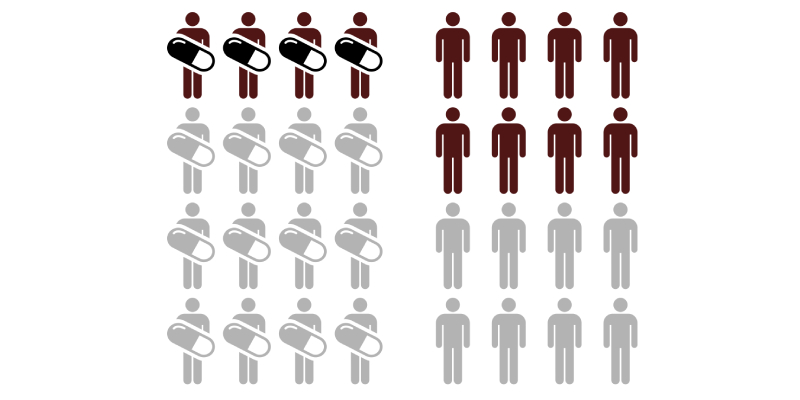
Around the world, 360 million people have moderate to profound hearing loss. Half of these cases of hearing loss are estimated to be avoidable. According to a recently-released news report from the World Health Organization (WHO), “some 1.1 billion teenagers and young adults are at risk of hearing loss due to the unsafe use of personal audio devices, including smartphones, and exposure to damaging levels of sound at noisy entertainment venues such as nightclubs, bars and sporting events.” Physical and mental health, education and employment are all significantly impacted by hearing loss. Studies from middle- and high-income countries were analyzed by WHO indicated that among teens and young adults aged 12-35, nearly 50% are exposed to unsafe sound levels from personal audio devices and almost 40% are exposed to potentially damaging sound levels at entertainment venues.
As noted by Dr. Etienne Krug, WHO Director for the Department for Management of Noncommunicable Diseases, Disability, Violence and Injury Prevention, “As they go about their daily lives doing what they enjoy, more and more young people are placing themselves at risk of hearing loss. They should be aware that once you lose your hearing, it won’t come back. Taking simple preventive actions will allow people to continue to enjoy themselves without putting their hearing at risk.”
Recommendations by WHO experts say that the highest permissible level of noise exposure at work is 85 dB up to eight hours each day. Because nightclubs, bars and sporting events typically have noise levels of 100 dB – a level that is safe for only about 15 minutes. Suggestions for teens and young adults for hearing protection include:
- Keeping volume down on personal audio devices,
- Wearing earplugs when visiting noisy venues,
- Using carefully-fitted, noise-cancelling earphones or headphones,
- Limiting time spent in noisy activities by taking short listening breaks,
- Restricting daily use of personal audio devices to less than an hour,
- Using smartphone apps to monitor safe listening levels,
- Heeding warning signs of hearing loss and getting regular hearing check-ups.
In addition to personal efforts to protect hearing better, other useful initiatives include:
- Developing and enforcing strict legislation on recreational noise,
- Raising awareness of risks of hearing loss with public information campaigns,
- Educating young people about safe listening,
- Managing entertainment venues by using sound limiters, offering ear plugs and “chill out” rooms,
- Designing personal audio devices with safety features,
- Displaying information about safe listening on products and packaging.
“To mark International Ear Care Day, celebrated each year on March 3rd, WHO is launching the “Make Listening Safe” initiative to draw attention to the dangers of unsafe listening and promote safer practices. In collaboration with partners worldwide, WHO will alert young people and their families about the risks of noise-induced hearing loss and advocate towards governments for greater attention to this issue as part of their broader efforts to prevent hearing loss generally.”